Low back pain and rib stress injuries are two of the most common and costliest rowing injuries. Low back pain (LBP) affects 32-53% of rowers and is the leading cause of missed training sessions. Rib stress injuries (RSI) affect fewer rowers, more like 10%, but as a bone injury, the recovery time is much longer. A typical recovery window is 3-8 weeks of rest, rehab, and gradually returning to rowing. It is critical to understand and reduce risk factors for these injuries, because previous injury is one of the biggest risk factors for future injury. Once you get one, it’s more likely to get another, so we have to start with reducing risk, then preventing the first injury, then reducing injury rates overall.
Warning: This article is long, at nearly 6,000 words, and heavily sourced with the most up-to-date research on low back pain and rib stress injuries in rowers. I originally wrote this as a final paper in my graduate school biomechanics class, and adapted it to blog format with the goal of creating a comprehensive, accessible resource for rowers, rowing coaches, and strength coaches of rowers.
My goal with this article is to provide specific education for the rowing coach, strength coach, and rower detailing the mechanism of injury, risk factors, and rowing and strength training strategies to reduce LBP and RSI in rowers. You can use the links below to jump straight to a section as well.
- Limitations of Research
- Injury Mechanism: LBP
- Injury Mechanism: RSI
- Risk Factors: LBP & RSI
- How Coaches Can Reduce Rowing Injuries
- How Strength Coaches Can Reduce Rowing Injuries
- How Rowers Can Reduce Rowing Injuries
- Wrapping Up

Limitations of Research
Research provides trends and general information based on the study methods, population of participants, and thoroughness of the researchers. Research does not provide definitive, concrete, absolute answers, nor does it deal in individualized prediction or prescription. Coaches and practitioners then take this general information and learn to apply it to specific athletes and situations to dial it in to the individual level. Research does not provide definitive or prescriptive answers, such as “you must do X,” or “you must not do Y.” We can use research to understand trends, general principles, and risk factors, and then combine this with our own personal experience and knowledge to determine the best approach for our specific coaching or training context.
Rowing research around LBP and RSI has a few additional limitations. The biggest one is that the majority of the research is done on ergs, usually static ergs. In most cases, we are left to speculate as to the effects of on-water rowing. A second limitation is that the sport of rowing encompasses a wide range of individuals from juniors to masters, rowing single sculls to sweep eights, around the world. All of these variables affect the technical and training program style, needs, execution, individual effects, and research applications. Finally, researchers still do not absolutely understand the exact mechanisms of injury for either LBP or RSI. I will reference the dominant theories as to how and why these injuries occur, but they are just theories and more research is needed to understand the injuries so we can develop strong evidence-based training practices for training, recovery, and rehabilitation.
Injury Mechanism: Low Back Pain in Rowers
When we talk about LBP, we’re talking about non-specific LBP, which is general pain in the lumbar spine area that is NOT an injury to a disc, ligament, facet joint, or specific muscle. Non-specific LBP is the aching, chronic kind of pain that you might get some relief from after stretching or walking around, but comes back around training sessions, and usually doesn’t have one clear cause of injury.
LBP affects 32-53% of rowers in 12-month studies and research indicates that this type of chronic pain is most often related to technique and training volume. Rowing is a cyclical movement pattern and the high training volume typical of endurance sports results in hundreds of repetitions of the stroke cycle during a typical training session. Rowers must accurately and consistently translate physical strength and endurance to a refined technique to produce boat motion, and technical deficiencies add up quickly in this environment to have a big effect on performance and physical health.
Multiple studies (one, two, three) found that prolonged static erg sessions (defined as 30+ minutes continuous) resulted in technical breakdown that caused increased flexion and extension as well as side-to-side motion at the lumbar spine vertebrae. Basically, as rowers approach and continue past the 30-minute mark, the lumbar spine begins to move past its normal rowing stroke range-of-motion. More flexion (rounding) on the recovery or at the catch means more extension (arching) on the drive and at the finish. In addition, researchers found angular displacement, or side-to-side motion, at the lumbar vertebrae as rowers rowed longer and closer to maximum output. This occurred particularly on the recovery and at higher rates, which suggests balance problems possibly the result of fatigue. This increased lumbar spine motion occurred in novice, collegiate, and elite rowing populations, and it’s bad for two major reasons.
First, to maximize transfer from training to performance, erg work should be performed as technically similarly to on-water rowing as possible. The more different erging is from on-water rowing, the less carryover the athlete will get from training to performance.
Second, these changes result in less lower body and more upper body contribution to the stroke. Static ergs already have a higher peak force at the handle than dynamic ergs or on-water rowing, as well as greater muscle activity in the upper body. As lumbar flexion and extension increases under prolonged rowing conditions, the rate of force development decreases and the athlete reaches peak force later in the stroke cycle. This shifts the power production emphasis even further away from the legs, and more onto the back and shoulders.
One study of 13 national and international-level male rowers described the cascade of effects from prolonged rowing and altered spine kinematics as such:
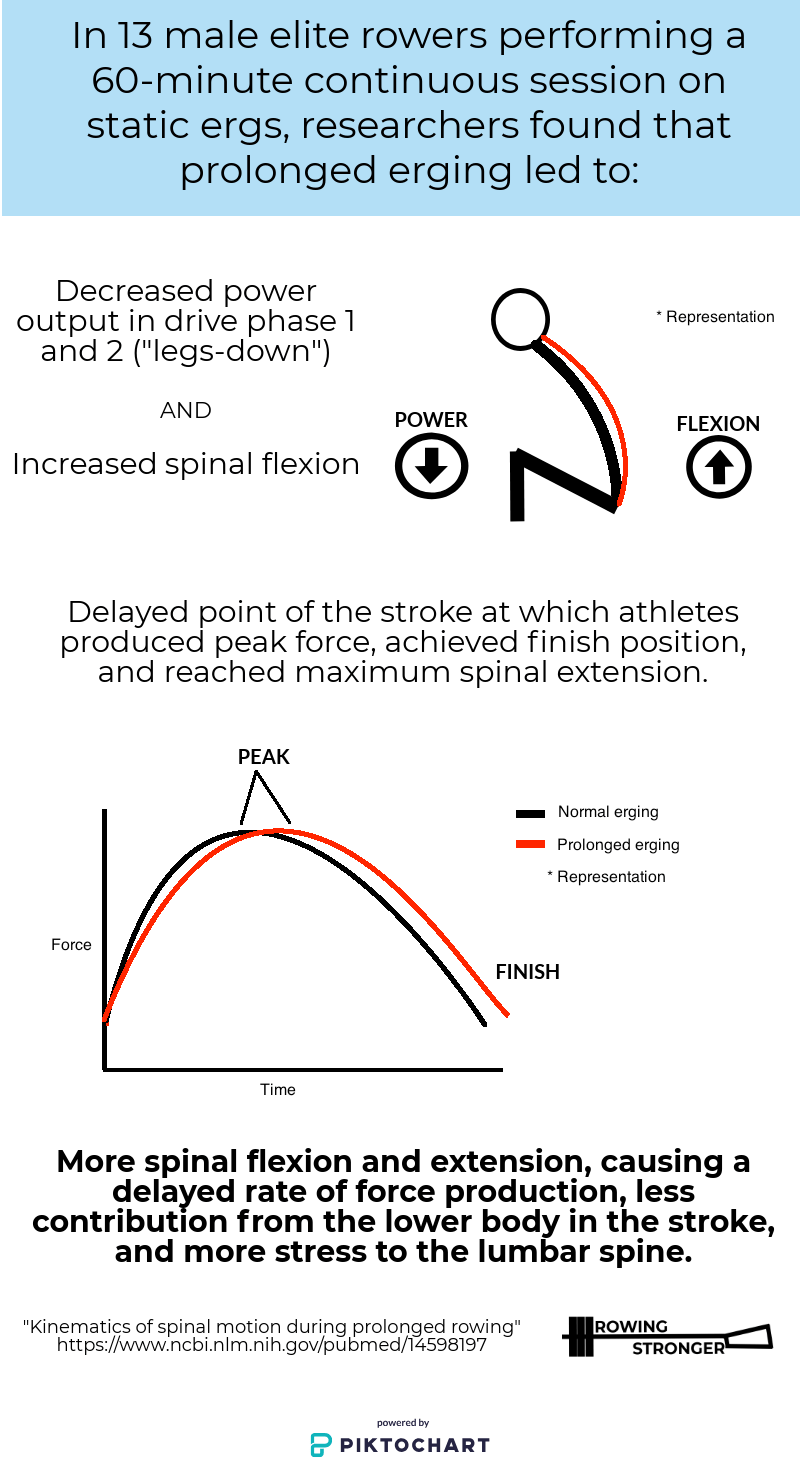
- Decreased power in drive phase 1 and 2 (early drive, the “legs-down” phase)
- Delayed point of the stroke at which peak force was achieved
- Delayed point of the stroke at which finish position was achieved
- Increased magnitude of spinal flexion
- Delayed point of the stroke at which maximum spinal extension was achieved
Click the infographic on the right for a visual representation of this study.
The current proposed mechanism of injury is that this increased stretching and loading of passive (ie. non-muscular) spinal structures can lead to tissue strain and chronic pain. Right now, this is as close as we have to a dominant theory as to why non-specific LBP is painful. Increased range-of-motion results in increased force. This increased force is exerted on structures that aren’t prepared to handle high force, and this leads to pain.
Injury Mechanism: Rib Stress Injury in Rowers
Rib stress injury (RSI) is a catch-all term describing a spectrum of overuse injuries causing pain to the chest area. RSI affects around 10% of rowers and includes strains, stress fractures, and full fractures. These injuries occur as a result of the bone’s failure to remodel itself following microdamage from continuous mechanical loading. In simple terms, the ribs experience loading throughout each rowing stroke. If the bone doesn’t heal itself adequately following each session, more and more strokes cause more and more microdamage that the bone can’t recover from, and an injury occurs. While RSIs affect fewer rowers, the time for recovery is much longer, with one study of Australian rowers recording an average of 47 lost days of training for a low grade RSI and up to 60 for a full stress fracture.
RSI are multifactorial, meaning that there isn’t one single cause of injury, but a panel of significant risk factors and aggravating incidents that may lead to injury. There are a few theories of mechanism of injury, the most well-supported of which is the rib cage compression theory. The idea here is that the mid-drive phase is where the highest peak force occurs, as does the resultant force vector of arms to oar handle and the scapular retractor muscles, which creates a compression force on the posterolateral (rear-and-outside area) rib cage. Mid-drive phase coincides with the highest reported pain in RSI rowers, and researchers have found higher co-contraction of scapular muscles in RSI rowers compared to a matched control group, suggesting that RSI rowers experience higher forces acting on the ribs during the drive phase.
I studied these injuries together because what happens at the spine affects what happens at the rib cage. The rowing stroke is a cycle, and we cannot isolate one element or error and expect it to only have an effect on that specific movement or stroke phase. All of the force developed in the lower body has to go through the rib cage, shoulders, arms, and wrists in order to get to the handle and blade and create stroke motion. The increased spinal motion from prolonged erging or poor technique decreases the lower body contribution and increases the upper body contribution. This means more force on the rib cage, and an increased risk of RSI, as well as increased risk of LBP. LBP is itself a risk factor for RSI, as rowers experiencing LBP can develop technical compensations that result in greater upper body forces, and increased stress on the rib cage. We must treat these injuries as related.
Risk Factors for LBP and RSI Rowing Injuries
Researchers noted an increase in rowing injuries, including LBP and RSI, in the early 1990s, when hatchet blades and static ergs became popular and commercially available. Hatchet blades have a greater surface area and catch the water faster than the Macon, or tulip/spoon-style, blades that preceded them. Researchers suggest that the increase in force production without adequate strength to support the higher output is a risk factor for LBP and RSI. Concept2 static ergs became commerically available and popular in rowing programs in the late 80s and early 90s and have been increasing in popularity ever since, especially with the Crossfit boom. Before this time, even programs that had ergs rarely had enough of them for all rowers to engage in high volume training programs. Rowers tended to spend the off-seasons cross-training, lifting weights, or off entirely. Commercially available ergs facilitated year-round specific rowing training in the USA. Combined with hatchet blades, these technical changes greatly increased the training volume and training load for rowers at all levels. There is no doubt that the ability to increase per-stroke output and train specifically for rowing year-round also contributes heavily to the improvement in performance of the last 25 years, but researchers also note them as risk factors for LBP and RSI.
To be clear, static ergs are an excellent tool to enable rowers to train specifically for rowing year-round, in the off-season when rowable water isn’t available and in-season when lineups don’t work out perfectly. Ergs are great teaching tool for teaching novices, focusing on specific elements of the stroke, and getting lots of athletes lots of practice strokes when we’d previously be limited to rotations in a barge or tank. However, they come with the cost of significantly higher peak force on the stroke than on-water rowing or dynamic/sliding ergs. In one study of male and female collegiate rowers, researchers found that rowers using dynamic/sliding ergs decreased peak handle force by 14.8% compared to static machines. Researchers in another study found significantly greater muscle activity in the biceps, deltoids, and trapezius on static ergs compared to single sculling. More force, and more force from the upper body, means more stress on the lumbar spine and rib cage, which means more risk of LBP and RSI.

Prolonged rowing (30+ minutes continuously) on static machines is one of the most significant risk factors for both LBP and RSI. Nearly every research article examining erging and LBP (one, two, three) noted the increased ROM at the lumbar spine when rowing for 30-minute (or more) continuous pieces, increasing stretching and loading of passive spinal structures to cause tissue pain. Static ergs are a great training tool, but like any tool, only if they are used responsibly. Static ergs already exert higher peak forces on athletes and put more stress on the upper body than dynamic ergs or on-water rowing. Under prolonged rowing conditions, this increases even further as subconscious technical breakdown exerts even more stress on the spine and rib cage.
Training volume is one of the other most significant risk factors. In a study of over 1600 NCAA rowers, researchers found that LBP was most likely to develop during the winter season (39%) compared to spring (33%), fall (25%), and summer (4%). Those line up almost exactly with the amount of meters rowed and amount of time commonly spent on ergs. In a study of 76 elite rowers representing New Zealand, researchers found a high positive correlation between LBP prevalence and total training hours per month, total ergometer training hours per month, average training hours per participant per month, and average number of meters rowed per month. The authors also noted that a significant increase in new cases of LBP occurred in the month in which athletes returned to training from their off-season break and experienced a rapid increase in training load. High total training load, an accelerated path to developing high training load, and if training load is achieved with static ergometers, are significant risk factors for LBP and RSI.

Because RSI is a bone injury, low bone mineral density (BMD) is also a risk factor. Researchers have found that male and female lightweight rowers are at greater risk of disordered eating, intentional weight loss, calorie restriction, and low BMD than openweight rowers, and at greater risk of RSI. In one study of 21 elite female lightweight rowers, seven participants experienced rib pain and had significantly lower lumbar spine and total body BMD than those who did not. The “female athlete triad” used to be the term for inadequate calorie intake relative to energy expenditure causing impaired menstrual function and low bone mineral density. Researchers from the International Olympic Committee redefined this in 2014 as the “Relative Energy Deficiency in Sport,” or RED-S, to reflect the fact that male athletes and female athletes alike engage in calorie restriction, are at risk for disordered eating, and that menstrual function is just one of many physiological functions impaired from inadequate calorie intake including immune system, metabolic rate, protein synthesis, psychological and cardiovascular health, and more.
Weak knee extensors (quadriceps) may be a risk factor for RSI, and weak knee flexors (hamstrings) are a risk factor for LBP. Researchers in one study found that rowers who had previously had an RSI had a lower ratio of strength between knee extensors and arm flexors, compared to matched controls of rowers without RSI history. The RSI rowers were proportionately stronger in the upper body and weaker in the lower body. RSI rowers may row a stroke that is heavier on the upper body, exerting more strain on the rib cage, leading to the injury. Researchers in another study found that a high ratio of quadriceps-to-hamstring strength was a risk factor for LBP. The stroke does a great job of developing the quads, but a poor job of developing the hamstrings, and this imbalance may lead to LBP. I’ve done a detailed review of this study at the link below.
Read More: Is Hamstring Flexibility for Rowers Overrated?
Hip flexor mobility and thoracic mobility have interplay, and combined, can be risk factors for both LBP and RSI. If hip flexor mobility is restricted, athletes may compensate elsewhere to achieve stroke length. Most often, this comes in the form of lumbar flexion and thoracic protraction. A hip mobility restriction can preference the athlete into lumbar flexion, preventing thoracic extension without lumbar extension compensation. You can try this on your own by artificially restricting your hip extension (ie. bend forward as though hip hinging) and then trying to achieve an upright torso position in thoracic extension (ie. stand straight up and put your arms above your head). It should be impossible to do without hyperextending the lumbar spine to compensate.
This plays out similarly in the stroke. Tight hip flexors will prevent you from sitting up straight and rocking over at the pelvis. This results in poor recovery sequencing that begins with shoulder protraction and often excessive rounding of the spine, leaving the hips to play catch-up for the rest of the recovery. This sets up a sloppy, rushed catch with poor compression, poor hip and torso positioning, and poor bladework at the catch. A bad catch means an inefficient early drive, and now it’s the back end of the stroke with pressure to make up, so with the legs ineffectively halfway down, the rower swings hard with the upper body, diverting more stroke force through the upper body and increasing rib cage pressure. I demonstrate these compounding errors below.

From Hume, McDonnell, and Nolte (2011):
“It is also important to pay particular attention to the kinetic chain distal to the site of injury. Lack of flexibility in the lumbar spine and hips shortens the stroke, and may cause an individual to compensate by altering scapular protraction. Excessive protraction alters the resultant force between retractors (rhomboid muscle group) and the combined water resistance on the oar, leading to abnormal posteriorly directed forces on the rib cage.”
Reducing Rowing Injuries in Rowers
A quick recap:
- LBP is a chronic injury and occurs as a result of technical breakdown that increases ROM at the lumbar spine, stretching and loading passive spinal structures, resulting in tissue strain and pain.
- RSI is an overuse injury and occurs as a result of the bone’s failure to heal itself from mechanical loading experienced during rowing training.
- Prolonged (30+ mins) static erging is the most significant risk factor. The lumbar spine increases ROM, which leads to a delayed force production profile and greater peak forces generated from the upper body, which leads to increased stretching and loading of passive spinal structures to cause tissue strain and pain.
- Most of the other significant risk factors for LBP and RSI have to do with training load and volume. High training volume, especially when that high training volume is achieved rapidly and with static ergs, is a significant risk factor. High load per stroke comes from hatchet blades, static ergs, low rate training, high drag erging, rowing eights by pairs or fours, and/or added resistance rowing training.
- There is interplay between hip mobility and thoracic mobility that affects risk of both LBP and RSI, and can create confusion when attempting to provide an intervention to address hip and/or thoracic mobility.
- History of LBP and RSI is a significant risk factor. Once you have one, it’s more likely that you’ll get a second one in the future. We must start with reducing risk factors, to reduce the first injury, to reduce overall injury rates.
Now that we’ve laid out the mechanisms, causes, and risk factors for these two injuries, let’s get into the action plan for rowing coaches, strength coaches, and athletes, and how we can all work together to reduce risk of injury and enjoy more productive training sessions for a longer career.
How Coaches Can Reduce Rowing Injuries
There are several things that rowing coaches can do to be more aware of risk factors for LBP and RSI and put strategies in place to reduce risk factors.
#1. Minimize overlap of high volume and load
Look at your training program and evaluate sources of high training load.
- Low rate erging and rowing
- Rowing with hatchet blades
- Using only static ergs
- Rowing eights by pairs or fours
- Rowing upwind or upstream
- Added-load rowing via high-drag erging, bungee cord, boat weights, rigging, etc.
It is particularly important that we introduce high load rowing situations gradually, and minimize overlap of high training load and high training volume. For example, if we’re doing a phase of low rate work and rowing eights by pairs or fours, we should decrease load and volume elsewhere. Consider switching to sliding or dynamic ergs to reduce per-stroke load, or reduce the flywheel resistance on static ergs, or use cross-training instead of erging sessions. Perhaps we decrease volume across the board while we focus on higher load technical work.
I designed a flowchart of possible volume and load management strategies, available here (PDF).
#2. Plan for gradual increases
Using the above volume and load management strategies, implement a strategy to decrease and then gradually increase training volume and load at certain times of the training year. For example, when athletes return from summer break, use decreased load and/or volume training and then gradually increase from that point. The typical approach of jumping right back into training, or worse, a “training camp” of high load and high volume training to attempt to “make up for lost time,” is a significant injury risk.
#3. Cross-train for aerobic fitness
Prolonged training on static ergs is one of the most significant risk factors for LBP, and a significant risk factor for RSI. The aerobic adaptations we seek with long-and-low aerobic endurance training are more general and systemic. These are functions of the total body cardiovascular pathways, and can be trained effectively in ways that do not load the spine and ribs as forcefully and repetitively as prolonged erging.
Dynamic ergs may be preferable to static ergs. As of this writing, there have been no controlled studies comparing injury rates with static and dynamic ergs. All research on prolonged erging and injuries is on static ergs, so we do not know what technical changes occur in prolonged erging on dynamic ergs. The signs point toward dynamics being preferable for their lower per-stroke load and proportionately greater lower body contributions, but we do not have academic research on this.
If dynamic ergs are not available, then using cross-training such as cycling, swimming, or running may be a better option than prolonged static erging for aerobic fitness. Save your static erging for shorter distance, lower volume, higher intensity training that is more specific to rowing performance.
#4. Emphasize technique more than power output
Novice and experienced rowers alike demonstrate a drive to maintain power output, even if that means sacrificing technique. Technical degradation doesn’t just negatively affect carryover to on-water performance, it’s an injury risk for the two costliest rowing injuries. Consider using heart rate, rather than split, for more workouts to allow athletes to focus on maintaining technique under appropriate exertion, rather than maintaining output at any cost. Teach athletes how to achieve stroke length with lumbopelvic rotation, rather than flexion and extension of the lumbar and thoracic spine. Some spinal flexion is natural and desirable to effectively distribute load across the vertebrae, but the majority of the power of the drive and reach on the recovery should come from pelvic rotation.
#5. Include mobility work in rowing training
If you have a strength coach working with your program and including mobility in training, great. Work with them to identify ways that you as a rowing coach can emphasize the importance of mobility and recovery in rowing training. Many programs do not have strength coaches, or even strength training programs. These programs in particular should dedicate time to properly warming up for rowing training and including mobility work for the hip and thoracic area in their rowing training. This will introduce athletes to skills that they can use on their own, prepare their bodies for rowing training, and make some improvement in movement quality to achieve better positions in the stroke, reducing load on the spine and torso.
How Strength Coaches Can Reduce Rowing Injuries
The #1 priority for strength coaches is to build the athlete up against injury. Performance improvement is #2.
#1. Always supervise athletes
Strength training was noted in one study as a risk factor for LBP. However, strength training is also a research-recommended part of every rehab and prevention program. This suggests that quality supervision and instruction is the key to avoiding injuries in the weight-room as well as using strength training as part of an injury prevention protocol. Be aware of your coach-to-athlete ratio. Are we adequately staffed to supervise the load that athletes are using, their technique, and their movement quality?
#2. Educate and communicate
One key problem with RSI is delayed diagnosis. RSI symptoms can be difficult to pin down and describe, and RSI are often misdiagnosed as a cartilage or intercostal muscle strain. This results in delayed off-loading for the athlete, and a longer recovery window. Athletes often self-treat LBP with time off or avoiding certain exercises, which might be effective in the short-term, but it fails to address the root cause of the problem in the long run. We have an ability as strength coaches to be informed on the common injuries, common symptoms, and to serve as liaison between athletes, coaches, and other staff members to oversee the recovery protocol. We are also in position to educate on reduction strategies, such as nutritional information around RED-S, supplementation information around Vitamin D for bone mineral density, and recovery protocols to improve sleep, hydration, stress management, and reduce risk of injury.
#3. Teach the movements
Strength training offers numerous opportunities to teach movements that are relevant to the rowing stroke and can reduce risk of LBP and RSI. In addition to hip mobility exercises to improve range of motion, teach the hip hinge, Romanian deadlift, and kettlebell swing to help athletes improve lumbopelvic coordination. This will help athletes achieve length and power in the boat through the hips, rather than through the spine. Teach scapular muscle control (eg. batwing row, pullapart, YWT raise) and how to effectively transmit force through the thoracic muscles. This will help them maintain a strong shoulder position to distribute force throughout the torso, instead of concentrating it on shoulder protraction and retraction only. Use analogies to the rowing stroke to help athletes see the carryover of strength training skills to rowing skills.
Read More: Complete Guides to Individual Exercises
#4. Improve rowing-relevant muscle strength and mobility
Strength training for rowing plans should be specific to rowing performance, not bodybuilding, powerlifting, or programs from other sports. Include exercises to improve rowing performance, as well as exercises to target muscles that rowing fails to develop. For example, researchers in one study found that improving hamstring strength to balance quadriceps strength reduced the number of training sessions missed by LBP rowers. Although the mechanism isn’t fully understood, training the serratus anterior has been shown in research to improve RSI rehabilitation protocols and I include it in my injury prevention work.
Assess both hip flexor mobility and thoracic mobility. Assess them separately to attempt to rule-out interplay, as a mobility restriction in one can impair the other (see Risk Factors above). Include preventative mobility work for both as a routine part of strength training for rowing. I tend to “sneak” a lot of this work into my rowing warmup routines. I also try to work with the rowing coaches to include some of this work in their rowing training, as warmups, cooldowns, and land workouts.
#5. No Bench Pulls
Bench pulls and bench presses exert high force on the rib cage and researchers suggest that they be avoided for rowers at risk of RSI. “Rowers at risk of RSI” is a pretty broad category considering the risk factors noted in the Great Britain Rowing Team RSI Guidelines. The benefit gained from these exercises is not worth the potential cost of causing or aggravating an RSI, considering how many other exercises can be used instead.
How Rowers Can Reduce Rowing Injuries
There are at least 20 hours of the day when rowers are not under a rowing or strength coach’s supervision. During that time, you can increase or decrease your risk of LBP and RSI. Which would you rather do?
#1. Stick to the script
If the coach is being intentional about tracking volume, managing load, and progressing gradually, don’t mess that up by adding extra sessions on your own, pulling workouts at lower splits than prescribed, or adding sets and sets of additional strength training. If you think you should be training more, ask your coach for advice.
#2. Sleep, hydrate, and eat
These are the Big 3 of recovery. Before thinking about supplements or additional training protocols, are you taking care of the basics? Athletes who sleep less than 8 hours a night have 1.7 times higher risk of injury and are nearly 3 times more likely to catch a cold. Adequate hydration, and quality as well as quantity of nutrition are critical to muscular growth, total body health, and your ability to continue improving in training. Before you add more training, add more recovery and see what happens.
#3. Dedicate to technical mastery
Rowing is a sport of power, endurance, strength, and fitness, as well as a sport of finesse to demonstrate all of those physical qualities through a highly refined technique. Remember this as you train on the water or on the erg, and seek to become a master of your craft. Just yanking on it for extra meters does little but improve aerobic fitness, and you can improve aerobic fitness on the bike even better without the risk of LBP and RSI.
Two More Ideas Worth Considering
There are two ideas that I think are worth considering as LBP reduction strategies. Neither one currently has research behind it, which holds me back from including them in the above evidence-based strategies. I hope that these will be evaluated by future research on rowers, because the ideas seem sound and they are low-cost interventions that anyone could add to their training.
The first is a World Rowing blog by rower and chiropractor Bob Cummins. Cummins proposes his idea that when you DO do prolonged erging, take a 60-second break every 10 minutes to stand and stretch before getting back on the erg. A 60-second rest will have almost no effect on heart rate or training economy, and the advantage is the possibility that the quick break will facilitate some recovery of spinal structures and mitigate the damage from prolonged erging. As of now, it is just a possibility. The advantage of this recommendation is that it can be immediately implemented with no extra equipment. The downside is that there isn’t research on whether or not this actually does help, so I’m hesitant to recommend it and lead people to believe that prolonged erging can be done safely until there is more research on it.
The second comes from another World Rowing blog, this one by rowing researcher and LBP specialist Fiona Wilson. Dr. Wilson wrote three of the research articles and reviews featured heavily in this piece, and I’m grateful for her work in the field. She suggests that isometric core exercises are not effective for developing core stability in rowers and preventing LBP, and that an approach that focuses on dynamic trunk extension endurance is more effective. She discusses this more in Joe Deleo’s podcast, starting about 38 minutes in.
I would like to see both of these approaches evaluated by research and will update this section if anything happens on that in the future.
Wrapping Up
LBP affects 32-53% of rowers and is the leading cause of missed training session frequency among rowing injuries. RSI affects around 10% of rowers and causes the most missed total training time, with recovery periods up to 3-8 weeks. The major proposed mechanism for LBP is increased flexion, extension, and frontal plane angular displacement of the lumbar spine as a result of prolonged continuous training sessions and extreme exertion causing tissue strain and chronic pain in the lumbar area. There are three major mechanisms of injury for RSI, with the most research currently supporting the rib cage compression theory that high contraction of the serratus anterior and trapezius muscles during the mid-drive phase of the stroke exerts bending forces on the rib cage. When combined with other risk factors, this cyclical compression can cause a range of rib injuries from strain to full fracture. Both LBP and RSI are overuse injuries and share similar risk factors for injury, including training volume, rapid increases in training load or training volume, prolonged use (>30-minutes continuous) of static ergometers, and poor lumbopelvic control, coordination, and ROM.
Rowing coaches may be able to reduce risk of these rowing injuries by emphasizing good technique over total power output when training on ergometers. Train the aerobic system with dynamic ergometers, or cross-training if dynamic ergometers are not available, rather than use static ergometers, to reduce lumbar tissue strain and rib cage stress. Finally, consider implementing a gradual progression of training volume and load when athletes return from the off-season or time away from regular, structured rowing training. Strength coaches should consider the hamstring-to-quadriceps strength ratio in regards to LBP and the knee-extensors-to-elbow-flexors strength ratio with regard to RSI. A strength training program that emphasizes hip ROM, lumbopelvic coordination, and strengthening of the anterior and posterior lower body as well as serratus anterior, thoracic spine, and trunk muscles may reduce risk of LBP and RSI. There is a lack of research determining evidence-based practices for rowing and strength training to reduce rowing injuries, and a great practical and ethical need for more research to understand mechanism of LBP and RSI, as well as rowing and strength training practices for injury management, rehabilitation, and prevention.
Last updated January 2019.

Get Rowing Stronger!
“Rowing Stronger: Strength Training to Maximize Rowing Performance” is the comprehensive guide to strength training for rowing, from first practice of the off-season all the way to peak championship race performance, and for everyone from juniors to masters rowers. The second edition is available now in print and e-book.

Hi Will,
I can’t thank you enough for making this available to the general rowing community. It’s quote an impressive article and it will take multiple readings to gather the full depth of the info available. Definitely one for the ages.
Thanks Again,
Jeff Kirby
Thanks, Jeff! I’m glad you enjoyed it.